How many times should a child write a day?
There is no clear data on how much a child should urinate per day. In response to your complaint that your child rarely goes to the toilet, the pediatrician can only advise you to monitor the amount of fluid intake. But let's speculate based on real observations of preschool children.

At 3.5-5 years old, a child can tolerate 3-5 hours without a potty, then with this regime he can go to the toilet 3-5 times a day. But these data are purely theoretical, since you need to look at fluid consumption. If you think that your child does not go to the toilet well, then you need to monitor how much water, tea, compote, fruit juice, milk, and liquid from first courses he consumes per day.
For example, in maternity hospitals, children are allowed to drink boiled water 1-2 times a day (no more than 30 ml) between feedings. Pediatricians also say to give water to a child up to a year 1-2 times a day (no more than 60 ml), especially during periods of illness or heat. But one child can drink water with great pleasure, while another prefers to drink a liter of milk per day.

In summer or in a stuffy room, children drink more often and more, and in winter or in a ventilated, humidified room, accordingly, the volume of liquid they drink is less. In this case, of course, there is no reason to worry if the child does not go to the toilet very often. That's why moms should monitor their fluid intake before panicking at the pediatrician's office.
How to determine that a child does not go to the toilet a lot?
- Keep a diary for one week where you will write down what your child ate and drank during the day.
- Record how many times your baby goes to the toilet. It is best to measure the volume of urine during observations, as is done in the maternity hospital. To do this, pour the urine from the pot into a measuring glass and record the data in a diary.
- Monitor your child's well-being and record mood swings hourly in a diary.

Weekly observations will be enough for the pediatrician to see if there are any deviations in the baby’s development. Any doctor will tell you that if the baby is cheerful, cheerful and energetic, then there is no reason to panic. If a child does not go to the toilet a lot, and this bothers him, causes pain, causes whims and mood swings, then you need to contact a pediatrician, urologist, surgeon and get tested.
Home > Consultations > Pediatrician > Rare urination in children. Causes
Children never have stable physical indicators, and the younger the child, the more they can vary. At a certain age, a child may urinate quite rarely. In such situations, most parents wonder: what’s wrong with the baby’s health?
When looking for the reasons for rare urination in a child, you should start with an understanding of the process itself and its norms.
Urination is the process of filtering and removing urine from the body through voluntary muscle contraction and emptying the bladder. There are two important processes in urination - filtration and absorption (suction). The quality of urination depends on the activity and coherence of these processes.
The frequency of urination varies among different age groups. Human kidneys are one of the few organs that can develop outside the womb. The renal cortex and medulla can develop over several years, and the above-mentioned processes of absorption and filtration occur with their own characteristics in each age period.
Intermittent urination in a child is a reason to contact a specialist. Do not hesitate, since any acute pathology of the urinary tract leads to increased intoxication of the body and can be complicated by acute inflammatory processes in other organs and systems. In addition, untreated pathology of the kidneys and urinary tract often develops into a chronic condition and worries a person throughout his life.
To understand the facets of pathology, you need to understand what is considered normal. According to data adopted by the WHO (World Health Organization), the norms for urination in children are as follows.
| Child's age | MI frequency is normal, once a day |
| 1–5 days of life | 4–6 |
| Up to 6 months | 20–25 |
| 6-12 months | 15–20 |
| 1–3 years | 10–12 |
| 3–5 years | 7–10 |
| 5-7 years | 7–10 |
| 7-9 years | 7–10 |
| 9–11 years | 5–7 |
| 11–13 years old | 5–7 |
Accordingly, a decrease in the frequency of urination compared to the lower limit of the age norm can be considered rare urination.
When considering this issue, it is necessary to highlight two main criteria - the child’s age and physiology. If everything is relatively clear with the first, then the second may raise questions.
The physiological nature of the problem of rare urination is caused by reasons not related to the child’s illnesses. Pathological is the opposite of physiological, indicating the presence of a disease.
Further, the causes of rare urination in children will be considered from the point of view of both criteria.
Physiological reasons
2. In the period from 6 months and beyond, the cause may be either a physiological change in the rhythm of urination in the child or a violation of the diet. In the latter case, you need to adjust the calorie intake and the amount of fluid consumed.
3. Any infectious disease, not only inflammation of the urinary tract, can be accompanied by a significant decrease in urination. High body temperature, leading to dehydration, and as a result, rare urination. Insufficient fluid replacement when it is lost will not allow the body to get rid of toxins. That is why everyone knows the statement that in case of illnesses with high fever, you need to drink as much as possible.
Pathological causes
They most often explain precisely urinary retention - the inability to empty the bladder independently (which is called urinary retention).
There are more than a dozen reasons why this rather painful condition can occur. This is for adults. In children, there are much fewer such reasons, but unlike adults, the contractile capabilities of the bladder in children are relatively small, so urinary retention is much easier to cause.
Urinary retention can occur due to a number of very diverse reasons:
- obstructions to outflow from the bladder;
- inflammatory processes in the urinary tract;
- diseases of the nervous system;
- factors of a toxic or reflex nature.
Among the reasons that prevent the outflow of urine from the bladder are kidney diseases, both congenital and acquired.
Parents, as a rule, learn about congenital pathologies in the first months. Eg…
The child is already a day old, but he has not urinated even once? It is imperative to inform the doctor about this; most likely, when examining the penis where the external opening of the urethra should be, the doctor will find a small depression covered with a thin film - this is an unresolved remnant of the embryonic urethra. It is removed with a fine-pointed instrument, and the child urinates immediately.
Also, congenital phimosis can cause difficulty urinating in young children. Usually, mothers themselves draw the doctor’s attention to this cause of urinary retention - they say that during urination the child tenses up, becomes red, and one can see how his preputial sac is swollen with urine. This occurs because the lumen of the external opening of the preputial sac is narrower than the lumen of the urethra. In case of infection, with acute balanoposthitis, difficulty urinating becomes even more pronounced as a result of swelling of the mucous membrane of the foreskin. Some children experience complete anuria.
And among the acquired ones is paraphimosis - wrapping of the foreskin with pinching of the head of the penis. At the same time, the foreskin noticeably expands; in the suprapubic region, when stroking, a full bladder is felt. In this case, urine is either retained or released intermittently, in small portions. The diagnosis is made without difficulty. Another reason for urinary retention is some kind of obstruction in the urethra. This condition can be caused by a number of reasons... For example, a bladder injury. Children are careless in games. Therefore, a blow to the perineum during a game of football or a fight, even without visible signs of damage to the urethra at first (urethrorrhagia!), can cause acute urinary retention several hours later due to the development of edema. Also, obstruction of the outflow can be a blockage of the urethra with a stone. Some causes are typical for children, for example, urinary retention in young boys after forced stretching of the congenital narrow foreskin and simultaneous destruction of congenital adhesions between the foreskin and the head, as well as after dissection of the narrow external opening in mild forms of hypospadias. Acute retention occurs here in response to severe pain during the first attempts to urinate after the intervention. Rare causes of urinary retention in boys include tumors of the bladder (myxosarcoma) and prostate gland (sarcoma). In these cases, the condition is accompanied by severe pain when urinating. Urinary retention due to compression of the urethra can occur with tumors arising from the pelvis; Anuria rarely occurs with congenital urethral stricture.
Urinary tract infections
They are characterized by intermittent rather than rare urination in the child. In young children, urinary retention can occur due to a number of acute infectious diseases. In young children, acute cystitis often develops in a peculiar way. If acute cystitis in adults is accompanied by a frequent urge to urinate, then in childhood it can cause acute urinary retention. From the stories of the parents, it turns out that the child complains of pain in the lower abdomen, does not urinate, cries when he is given a potty, and holds his penis with his hand (if we are talking about a boy). When trying to palpate the abdomen, a small patient, due to pain, cries and strains the abdominal wall, as a result of which it is not possible to determine the distended bladder. The urine of children with acute cystitis is often blood-stained, which can lead to an erroneous diagnosis of acute nephritis (which is also facilitated by false albuminuria). Inflammation of the kidneys or nephritis is characterized by a sharp decrease in the amount of urine excreted and a change in its color - due to the increased number of leukocytes, it becomes cloudy. Other signs also appear: swelling of the face, body and limbs, severe lower back pain, low-grade fever.
Often, urinary retention in children depends on diseases of the nervous system, in particular the spinal cord. Most often this occurs when the spinal cord is compressed in patients with tuberculous spondylitis, spinal trauma, or myelitis. Both urinary retention and incontinence occur in acute meningococcal and tuberculous meningitis. Blum and Gohvard described such cases in two boys aged 13 and 15 years due to foci of poliomyelitis in the sacral spinal cord. Problems with urination in children can also arise due to injuries to the spinal cord and brain (concussion, fracture). In such cases, the child is given a bladder catheter for the entire period of recovery and treatment of the injury. Also, hysterical seizures can cause both urinary incontinence and acute retention. Elimination of the seizure or neurological syndrome resumes spontaneous urination. In this case, symptoms characteristic of neurological pathologies will be observed - tics, paralysis and paresis. With mental disorders, disturbances of consciousness and behavior immediately catch the eye.
Reflex urinary retention in children occurs in a variety of conditions. Long forced abstinence from urination. After it, a reflex spasm of the bladder and urinary canal occurs, which causes urinary retention in children. Often this condition goes away on its own, but if it lasts a long time and causes severe pain, catheterization of the bladder is resorted to. In this case, painful urges and tension in the walls of the bladder, felt as a spasm, may occur. Reflex urinary retention can occur with acute appendicitis, helminthic infestation (for example, ascariasis) and a number of other reasons.
It is clear that without finding out the root cause of this condition, it is difficult to provide significant help to a suffering person. We can only talk about temporary relief. And this is exactly what needs to be done before the doctor arrives, who will decide what to do next (place a catheter, examine, prescribe an examination, etc.).
Help from adult non-specialists with urinary retention accompanied by pain may include the following.
- Don't feed the baby. If he is very hungry, then offer a piece of an apple - no more.
- Offer to drink little by little (sweet tea or 5% glucose solution).
- You can try to relieve an acute pain attack and try to relax the bladder by placing the child in a warm bath with the addition of potassium permanganate.
- Give your child a tablet of no-shpa or papaverine - this will at least temporarily relieve the pain.
- Traditional medicine has in its arsenal many tools that help in such situations. Tinctures, decoctions, consumed internally and applied externally; baths with the addition of certain medicinal herbs - all this is possible and helps, but only in cases where it is reliably known what exactly causes this condition. Do not panic and, eager to help your child, start experimenting on him - wait for the doctor. Let him find out the cause and prescribe adequate treatment. Remember that the main principle of any medicine (and folk medicine too) is to do no harm!
If urinary retention is not painful
- You can try to provoke it with warm sitz baths and the sounds of flowing water.
- If a child has urinary disorders, the first thing you need to pay attention to is nutrition and water consumption. Not every liquid is equal to water, so it is worth teaching your child to drink regular clean water regularly. Fatty and spicy foods, as well as fast carbohydrates and coffee, which tend to retain fluid in the body, should be excluded from the diet.
All of the above remedies for urinary retention provide only a temporary effect, so always call a doctor.
Often parents, when the baby pees little, sound a premature alarm. Let's try to understand the norms and other indicators of this process.
Features of urination in children
State budgetary educational institution
higher professional education
Kuban State Medical University
Ministry of Health of the Russian Federation
Department of Pediatrics No. 1
Specifics of child care in connection with the anatomical and physiological characteristics of the organs of the urinary and urinary system.
Prepared by a student
1st year, pediatric faculty, 4th group
Voronina Alina Antonovna
Teacher Baum Tamara Givievna
Krasnodar, 2018
Content.
1.Anatomical and physiological features of the urinary system in children
2. Peculiarities of urination in children
3. Features of urine collection in children
4. Instrumental studies for kidney disease
5.Additional general clinical research methods
6. References
Anatomical and physiological features of the urinary system in children
At the time of birth, kidney maturation is not yet complete. The glomeruli in newborns are significantly smaller than in adults; their filtering surface is 30% of the adult’s norm. The tubules are shorter and narrower. Compared to adults, urine reabsorption in children is reduced.
With age, the urinary organs change. In young children, the size of the kidneys is relatively larger, the ratio of their mass to the body weight of a newborn is 1: 100, in an adult it is 1: 200.
The upper pole of the kidney is located at the level of the XI-XII thoracic vertebra, the lower - at the level of the IV lumbar vertebra. By 2 years, these features of the location of the kidneys disappear. In the following years, the growth of the kidneys corresponds to the growth of the body.
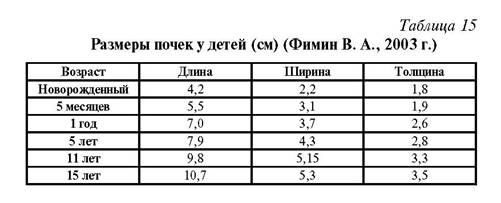
In the first years of life, the kidneys have a lobular structure. The cortical layer is underdeveloped. The glomeruli of a newborn are compactly located. The amount of glomerular filter in children in the first months of life is reduced due to the fact that their filtering surface is much smaller than in adults (see Table 15).
As the bud grows, uniform development of the fronts is observed.
The amount of urine produced in a child can normally be approximately calculated using the formula:
V = 100 x (n + 5), where V is the volume of urine per day;
n is the number of years.
Or according to the formula:
V = 600 + 100 (n – 1),
where V is the volume of urine per day;
n is the number of years.
Children need more water to eliminate toxins than adults. Dehydration occurs much faster in children. Babies who receive breast milk absorb it completely and there is very little product eliminated through the kidneys. In this regard, with low functional capabilities and imperfect systems regulating water-salt metabolism, the child maintains a constant internal environment. When replacing breast milk with other products, the load on the kidneys increases, the amount of products to be removed increases, the kidneys work under greater stress, and the acidity of the urine changes.
The kidneys are involved in maintaining the osmotic regulation of blood and extracellular fluid metabolism and maintaining acid-base balance.
Urine is formed as a result of the active function of the nephron, through which ultrafiltration of plasma occurs in the capillaries of the glomeruli; reabsorption of water and glucose occurs in the tubules, as well as the synthesis and secretion of compounds necessary for the body. Low molecular weight, water-soluble compounds pass through the glomerular filter membrane from the blood plasma. The kidney filter does not allow cellular elements and proteins to pass through.
Regulation of urine formation occurs through the pituitary gland, adrenal glands, humoral and nervous pathways. Water excretion is regulated by antidiuretic hormone. Aldosterone, a hormone of the adrenal cortex, increases the reabsorption of sodium and the excretion of potassium. In the first 3 months, 90 ml of urine is excreted per 1 kg of weight, at the age of 10 years - 25-35 ml per 1 kg of weight per day.
Ureters. The ureters in young children are relatively wider and more tortuous than in adults. The walls of the ureters are equipped with poorly formed muscle and elastic fibers.
Bladder. In newborns, the bladder is oval in shape and is located higher than in adults. Its mucous membrane is fully formed. As the child ages, his muscle layer and elastic fibers thicken. The capacity of the bladder in a newborn is 50 ml, in 1 year - 200 ml.
Urethra. In boys, its length is 5-6 cm, in adult men - 14-18 cm.
Features of urination in children
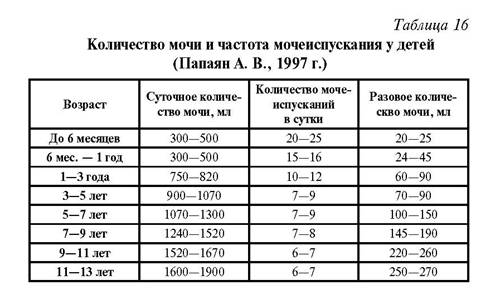
A newborn urinates due to innate spinal reflexes. Upon reaching the age of 12 months, the conditioned reflex to urinate is fully established (see Table 16).
The most informative indicator of the urinary system is a urine test. The color of urine is normally yellow; the color of urine depends on the concentration of urinary elements. It may change with methylene blue, riboflavin, and food pigments.
Freshly released urine is clear. Turbidity when standing urine depends on the presence of large amounts of salts, acidic elements, bacteria, mucus and fat.
Urine has a slightly acidic reaction, and with artificial feeding it is slightly alkaline.
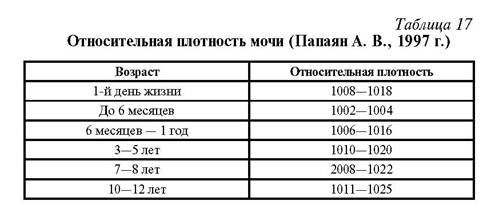
The density of urine ranges from 1002-1030. It depends on the amount of fluid you drink, your diet, and sweating. Urine in young children is less concentrated (see Table 17).
The density of urine is influenced by the presence of protein, glucose and other substances in it. A decrease in the relative density of urine is observed in chronic renal failure, pituitary failure and other diseases. An increase in urine density occurs with large fluid losses.
Urine sediment usually contains 1-2 squamous epithelial cells. During inflammatory processes, this indicator increases.
Columnar epithelial cells are found in the urine sediment in single numbers.
Red blood cells can be single: 0-1 in the field of view, up to 2 in girls.
Leukocytes are also found in normal urine 5-6 in the field of view.
Single hyaline and waxy casts can be detected in healthy people during physical activity.
Protein in the urine is detected during physical stress, inflammatory and chronic kidney diseases, when the permeability of the membrane filter increases.
Glucose in the urine can occur due to disturbances in water metabolism.
Ketonuria is detected with frequent vomiting and metabolic disorders.
An increase in the amount of urine (polyuria) is typical for patients with diabetes mellitus, chronic nephritis, during the discharge of edema, and after febrile illnesses.
Oliguria (a decrease in the amount of urine by 20-30%) or the absence of urine depends on a decrease or complete cessation of urine excretion by the kidneys, as well as on a reflex spasm and obstruction of outflow in the lower parts of the kidneys. Oliguria can be caused by heart and kidney diseases, fluid loss due to vomiting, diarrhea, or insufficient fluid intake.
Dysuria (impaired urination with urine retention in the bladder) is most often associated with a reflex spasm of the bladder sphincter in inflammatory diseases of the urinary tract, damage to the central nervous system and other diseases.
Pollakiuria (frequent urination) is observed in diabetes, chronic renal failure, and cooling.
Painful urination can occur with cystitis and other diseases of the urinary tract.
Along with a general urine test, a quantitative determination of red blood cells and white blood cells in the urine is performed. To do this, collect a daily portion of urine (Addis-Kakovsky test) or 1 ml of urine (Nechiporenko test).
Urinary standards for babies
The baby may pee for the first time during childbirth or immediately after it, or maybe after some time - even a day later. None of these indicators are considered a deviation from the norm. Later, the baby pees about 15 times a day, but if this happens less often, then you need to think about it.

On average, a baby produces about 200 milliliters of urine per day; a lower amount may be a cause for concern.
There are certain norms characteristic of each age:
- a newborn and a baby under 5–6 months of age should excrete from 300 to 500 ml of urine;
- from 6 months to 1 year – up to 600 ml of urine;
- from 1 to 3 years - in a volume of 780 to 820 ml.
This data gives parents an understanding of whether their baby is peeing sufficiently. Many nuances must be taken into account, for example, how the child eats, how active he is, and the ambient temperature. At the same time, low urine output may not always indicate any disease.
Daily diuresis in children: norm and causes of deviations
The peculiarities of the development of a child’s body are such that any diseases or pathologies progress faster than in an adult.
Due to immaturity, internal organs are more susceptible to inflammation and other negative effects, so you should carefully monitor the child’s health and pay attention to its main indicators. Daily diuresis in children is one of them.
Deviations from the norm indicate disturbances in the functioning of the urinary system and require a thorough examination.
general information
Daily diuresis is the amount of urine that is formed and excreted by the kidneys in 24 hours. This indicator depends on several factors:
- age;
- amount of fluid consumed;
- state of the urinary system;
- diseases of other organs;
- diet features.
Each age category has its own diuresis rate, and doctors take these limits into account when examining a patient. During the day, urine output is uneven, therefore, when calculating daily diuresis, daytime and nighttime diuresis are distinguished - the latter should be less. Deviations from the required indicators are a sign of problems with internal organs, not just the kidneys.
Thus, polyuria (increased amount of fluid) is more often observed in diabetes, both diabetes mellitus and diabetes insipidus. Oliguria (decreased urine output) develops with ascites, acute renal failure, intestinal disorders with profuse vomiting and diarrhea.
Anuria is an extremely small amount of urine production, no more than 50 ml per day. This amount is not even enough to fill the bladder. The causes of anuria are shock conditions, severe renal pathologies, and large blood loss.
Normal diuresis in children
Indicators depend on the age of the child. From 1 to 3 months, 170–590 ml per day is considered normal, at 4–5 months – 250–670 ml. From 7 to 9 months the norm is 275–740 ml, the average daily diuresis of a one-year-old child is in the range of 340–810 ml.
In children from one to 5 years old, 600–900 ml should be released in 24 hours; at 5–10 years old, the figure increases to 700–1200 ml. Diuresis in children 10-14 years old ranges from 1000 to 1500 ml.
This is the norm, but it is important to understand how much urine a particular child should produce. The determination is carried out using the formula 600+100(X-1), where X is the child’s age.
It must be taken into account that the amount of urine in children is influenced by many factors, not just age. Therefore, determining daily diuresis, although necessary at the slightest suspicion of disease, will not be the main diagnostic method. To make an accurate diagnosis, other types of examination will be needed.
Signs of impaired diuresis in a child
To start calculating the daily amount of urine, you need good reasons - symptoms that indicate problems in the baby’s body:
- bedwetting;
- elevated temperature;
- weakness, loss of appetite;
- pain in the lower abdomen.
These are signs of disturbances in the functioning of the kidneys, inflammation in them. But since changes in diuresis are recorded in various diseases, you should pay attention to other symptoms:
- increased thirst;
- sweating;
- swelling;
- vomiting and prolonged diarrhea.
It is imperative to determine diuresis in a child born after a difficult pregnancy if there was a risk of intrauterine development disorders. The counting algorithm in such cases is special; many factors are taken into account, including the degree of development and the functioning of other organs and systems.
What determines diuresis in babies?
Speaking about the factors influencing diuresis in a young child, it is necessary to remember that indicators going beyond the normal range are not always a sign of pathology. Thus, diuresis can vary depending on the maturity of the sphincter of the bladder and the organ itself, the urethra. If they are underdeveloped, then the bladder does not completely empty, although the kidneys work normally.
Urinary excretion is also affected by the timing of potty training. If you use diapers after a year, this interferes with the formation of the necessary reflexes, which also affects diuresis.
The diet of the baby or mother is of great importance if the child is breastfed. Salt retains fluid in the body, and many foods, herbal infusions, and medications have a diuretic effect. Therefore, before suspecting the worst, it is necessary to exclude all external factors. The disease cannot be diagnosed by the daily amount of urine alone!
How to collect urine
Urine is collected in one container - clean, with a volume of at least 3 liters. Usually a glass bottle or a special container with divisions is used. Throughout the day, starting at 6 a.m., the patient urinates only in this jar. The exception is the first urination in the morning, which occurs in the toilet.
The filled container is stored in a cool place. Throughout the day, the patient must adhere to recommendations regarding diet, drinking regimen, taking medications, personal hygiene, and rules for collecting material.
On the day of delivery, the collected urine is mixed and its quantity is determined. At least 100 ml of urine is poured into a separate container, and this container is sent to the laboratory for biochemical testing. When submitted to laboratory assistants, they announce the time period during which the material was collected and its daily quantity.
If urine collection is carried out from an infant, it is best to use special pediatric urine collectors. A child who already goes to the potty can control the process of urination, it is easier to follow the rules, but parents need to monitor the cleanliness of his genitals and the potty - not every baby can pee in a jar.
Source: https://nefrologinfo.ru/deti/sutochnyj-diurez-u-detej.html
Causes of rare urination
Let's consider the reasons when a baby pees a little, which is not confirmation of the presence of any disease:

- Excessive heat. Do not dress your child too warmly or heat up the room where the children are. This leads to dehydration of the body and, as a result, to low urine output.
- Insufficient amount of water in the diet. If a small child is already bottle-fed, then in addition to formula, he needs water.
- Transition from breastfeeding to artificial feeding. During this period, the baby urinates less, but there is no need to worry about this; short-term urination problems may occur.
- Hot and sultry weather. When the temperature outside is high, never forget to give your baby regular clean water.
- Diapers. After a child stops wearing diapers, problems with urine output may occur.
- Insufficient fat content of mother's milk. This factor most often affects before three to four months of age. How to increase the fat content of milk? Be sure to adjust your diet and introduce healthy fats into your diet.

If there are no reasons for low urination described above, then it is best to consult a pediatrician to establish a diagnosis.
What can parents do?
If urinary retention is not painful, you can try to provoke it with warm sitz baths and the sounds of flowing water.
If urination does not occur, you should call an ambulance to have the bladder catheterized.
If a child has urinary disorders, the first thing you need to pay attention to is nutrition and water consumption. Not every liquid is equal to water, so it is worth teaching your child to drink regular clean water regularly. Fatty and spicy foods, as well as fast carbohydrates and coffee, which tend to retain fluid in the body, should be excluded from the diet.
Urinary problems in children are not a cause for panic, but a cause for concern. Therefore, timely contact with a specialist is the main and first thing parents should do when such problems arise.
Author: Sukhorukova Anastasia Andreevna, pediatrician
Frequency of stool and urination in newborns
Not very abundant or infrequent urination in a child can be observed at any age. Considering the fact that the norms for this indicator change as the baby grows older, parents should familiarize themselves with the basic figures in advance. If it seems to the mother that her little one has begun to urinate little or rarely, you should not take rash independent actions, you should immediately consult a doctor and take all the necessary tests to make a diagnosis.

Only with the permission of a specialist can you use folk diuretics and even adjust the baby’s diet. According to statistics, all worries in most cases turn out to be in vain, or the condition requires only minor intervention.
What should you pay attention to if your baby is not urinating enough?
If there is sufficient fluid intake in the body and normal living conditions, the color of the child’s urine will be yellowish and translucent. Bloody spots in the urine pose a great danger. If the urine has a bright yellow color or dark shades, then this is confirmation that the child does not have enough fluid.
The time when a breastfeeding baby pees at night. If this does not happen, then, most likely, he does not have enough milk or the dose of artificial nutrition is incorrectly selected.

The ambient temperature is also important. If the room is too hot at night, moisture may leave the body through sweat, and the baby will not pee. On hot days, it is better to give the child more liquid or apply it to the breast more often.
Baby's nightwear should be made from natural materials and very light. Watch your artificial diet; it should not contain a lot of salt, which can cause little urination.
If there is a suspicion that the baby has problems with urine output, then it is necessary to observe his urination for several days. Then be sure to contact a medical facility and conduct diagnostic tests.
Home Treatment Options
In cases where the diagnosis allows us to exclude pathological processes, doctors recommend ensuring that the baby does not have a large amount of salty foods in his diet. Both newborns and adolescents should receive enough fluids per day. Its volume must be increased as the child’s activity or ambient temperature increases.
If the cause of the phenomenon turns out to be a pathological process, the approach to each child should be selected individually. Most often, in case of problems with the passage of urine in a normal volume or with the required frequency, the following manipulations are used:
- Sitz baths. Initially, cool water is used, then the temperature gradually rises.
- Compresses. Most often these are soothing compresses on the bladder area, but treatment of larger areas is also allowed.
- Medical nutrition. Food prepared for a child should not irritate the walls of the stomach.
- Douching. Used as an auxiliary method for painful emptying of the bladder.
Medications are prescribed only by a doctor. You should not hope that the baby will begin to write as it should if you give him a diuretic. Such actions can significantly complicate the situation.
Symptoms that may indicate the presence of the disease
Some symptoms should greatly alert parents, namely:

If the baby pees a little from time to time and no suspicious symptoms are observed, then, most likely, the individual characteristics of the baby’s body are manifested in this way.
If at least one of the symptoms is present in newborns, then under no circumstances should you self-medicate; you should definitely contact your pediatrician and undergo all recommended tests to identify the cause of rare urination.
Neurogenic bladder
Difficulty urinating in a teenager can be caused by other reasons besides inflammation. The act of urination can become uncontrollable if the genitourinary and nervous systems interact incorrectly. Spasms may occur. When there is an urge to defecate, urine is released with a delay.
The peripheral and nervous systems are responsible for the secretion of urine. If something is wrong, then the bladder cannot empty completely. Overflow occurs, and this causes the sphincter of the bladder neck to spasm even more.
If the spasm lasts for a long time, cervical cystitis may occur. The causes of neurotic spasms of the bladder include:
- neuroses;
- stress;
- prolonged urine retention;
- depression;
- panic attacks.
There may also be a disruption of connections between the organs of the urine excretory system and the nerve centers. This happens in severe cases. For example, with spasms caused by cerebral palsy, migraines, blockage of arteries, rupture of arterioles.
Currently, there are quite a few cases of pathologies in which degenerative processes begin, namely: urinary and fecal incontinence, delayed bladder emptying. This happens with multiple sclerosis.
What diseases may symptoms of infrequent urination indicate?
First of all, a small amount of urine may indicate that the child has kidney problems. It is this organ that is responsible for filtration processes, and if malfunctions occur, the kidneys immediately begin to reduce urine output.

Infectious diseases can cause urinary problems. Infections are especially dangerous under the age of 3 years.
The baby pushes when he pees, but at night he practically does not do this. It is possible that the baby has a pinched urethra or there are stones or sand in the genitourinary system.
Neglecting the doctor’s instructions in the process of treating other diseases, that is, using a large number of diuretics.
The general environment in the house is also important - if there is constant emotional stress, then the baby may experience problematic urination.

Phimosis is a disease that most often affects infants. The disease is characterized by a narrowing of the foreskin of the penis. The disease is most often hereditary, very rarely acquired.
Why does my baby pee often?
Modern parents
often try to look for problems where there really are none. For example, the most frequently asked questions from young mothers to the pediatrician are: “Why does my child urinate so often?”, “How much should a child pee per day?”, “Why does my child pee 3-4 times at night?” or, on the contrary, they are worried that their baby has begun to write rarely. Of course, every mother should be aware of the state of the child’s excretory system, but making a mountain out of a mountain when everything is in order with the baby’s health should not be done.
If the child is alert
, plays calmly, laughs, sleeps and eats well, then there is no need to worry about the frequency of his urination. Each child’s body is individual, and the fact that someone’s 1-year-old child pees 8 times a day cannot be the norm for your baby. Before sounding the alarm ahead of time, analyze what may be causing your baby’s urination problems. He may have eaten more than usual or drunk too much liquid.
After eating watermelon
, cucumbers, melons and other products with a diuretic effect, babies more often ask to go to the toilet. But if, in addition to frequent urination, the child develops fever, weakness, painful urination, swelling under the eyes, the color or smell of urine has changed, or if he complains of pain in the abdomen or lower back, then these symptoms indicate the development of a serious disease in the genitourinary system.
To clarify the reason, it is imperative
You should consult a doctor who diagnoses the disease based on the results of a general urine test. Any deviations from the norm in a general urine test are the first symptom of the development of an inflammatory disease or the presence of organ pathology; for a detailed study of disturbances in the functioning of the genitourinary system and the correct diagnosis, you need to take a urine test again according to Nechiporenko.
Frequent urination
can be considered if the baby begins to pee 2 times more often per day compared to the norm. So, normally a newborn child can write up to 20 times a day, children from 3 months to 1 year - up to 15 times a day, from 1 year to 3 years - up to 10 times a day, from 3- x years up to 9 years up to 8 times a day. And children over 9 years old, just like adults, feel the need to urinate up to 6 times during the day.
If the child does not urinate
for two days in a row and his bladder is empty, then urgently call an ambulance. A similar combination of symptoms is typical for anuria, which is a serious illness requiring immediate hospitalization. In addition to the absence of urination, with anuria the child turns pale, does not eat anything and sleeps for a very long time. Delayed initiation of treatment for this disease subsequently leads to convulsions and comas.

If the child
all urine tests are good, but he still feels the urge to urinate a few minutes after emptying his bladder, then most likely the baby is very excited during play or is experiencing nervous tension. For example, because of a quarrel between parents or punishment. In a state of stress, anxiety and nervous disorders, vasoconstriction occurs and a decrease in the delivery of oxygen to the body’s tissues. Our body compensates for the lack of oxygen by increasing urine production, so there is a desire to urinate more often than usual.
With this situation
Anyone who has taken an exam and experienced a strong desire to visit the toilet is familiar with it. In this case, you should not be afraid of frequent urination; pay attention to the amount and color of the child’s urine. If it is of normal color, and the portion of urine is not very large, then the child’s genitourinary system is fine. But in such situations, parents need to think about what worries the child so much and change their parenting methods.
If results
If a urine test is found to be normal, it is necessary to undergo a course of full treatment for the child. Most often, a child often pees with the development of the following diseases of the genitourinary tract: cystitis, urethritis, pyelonephritis, chronic renal failure, weakness of the muscles of the bladder walls and other pathologies. The most common pathology of the bladder is a symptom complex, which is called overactive bladder. It occurs due to disorders in the peripheral nervous system, as a result of which nerve impulses cause the bladder to contract frequently.
In this case, even if
There is a very small amount of urine in the child’s bladder, which signals the need to urinate. And, conversely, in the absence of the urge to urinate, the accumulation of a large amount of urine implies the presence of a pathology - a hyporeflex bladder. Also, children can often pee due to pelvic floor injury, diabetes and heart failure. These diseases always lead to the development of frequent urination. To clarify what causes urinary disorders in a child, it is necessary to do an ultrasound of the bladder and kidneys, and in case of injuries, conduct an X-ray examination of the pelvis.
If the child does not urinate
for two days in a row and his bladder is empty, then urgently call an ambulance. A similar combination of symptoms is typical for anuria, which is a serious illness requiring immediate hospitalization. In addition to the absence of urination, with anuria the child turns pale, does not eat anything and sleeps for a very long time. Delayed initiation of treatment for this disease subsequently leads to convulsions and comas.
Neurogenic bladder dysfunction
When a child's bladder does not perform its primary functions of collecting, holding, and emptying urine, it is considered hyperreflexive. This neurogenic pathology develops as a result of the immaturity of the nerve centers that regulate the normal functioning of the bladder.
Despite the fact that hyperreflex pollakiuria is a pathology, it does not cause discomfort. The urinary tract does not become inflamed, there is no pain or cramping during the process of urine excretion. The urge may intensify due to stress and colds. A hyperreflexive bladder often causes enuresis and incontinence.
When a child's bladder does not perform its primary functions of collecting, holding, and emptying urine, it is considered hyperreflexive. This neurogenic pathology develops as a result of the immaturity of the nerve centers that regulate the normal functioning of the bladder.
Types of examinations
All diagnostic measures are based on a single principle - from simple to complex. Therefore, to begin with, the pediatrician will prescribe a general urine test.
Even if the analysis does not give a real diagnosis, then it will still be possible to decide on further diagnostic methods:
- Urinalysis according to Nechiporenko. This study allows you to determine the number of red blood cells and white blood cells in the urine.
- Urine analysis according to Zimnitsky. Determines the exact amount of urine excreted by the baby throughout the day.
- Ultrasound or tomography are studies that allow us to study the anatomy of a child.
- X-ray using a contrast agent. The method allows you to determine the nature and speed of urination.
Ways to increase urine output
Before starting treatment, it is best to undergo a complete examination of the child’s body in order to completely exclude the possibility of diseases of the urinary system.

If pathologies are excluded, then you can resort to the following methods:
- give increased amounts of water to the child;
- almost completely eliminate salty foods from the diet;
- If the child has a high temperature or it is hot outside, then we also increase the amount of water in the diet.
Attention! Containing urination leads to the opposite effect: urine flows back into the ureters and other sections that are located above. If this happens constantly, ureteral reflux may develop, and in extreme cases, renal failure.
If inflammatory processes are suspected, it is recommended to take sitz baths daily and at the same time. Baths are taken while sitting; the water temperature should first be 27 ° C and gradually increase. You can use compresses that are applied to the lower abdomen or to the entire body. Douching can be carried out only as prescribed by a doctor and if there is pain when urinating.
Does your child rarely go to the toilet? This phenomenon occurs in children of all ages. Often the phenomenon can be eliminated after minor adjustments to lifestyle and nutrition. But it happens that rare urination becomes a sign of a serious illness. In what cases can a phenomenon be considered normal, and when does it indicate a pathology of the urinary system? What can parents do?
When should you sound the alarm if a child pees a little? Symptoms of serious illnesses in children
True, rare urination is not always harmless. There are a number of cases when a child pees very rarely due to illness, the presence of a serious pathology that requires immediate and thorough examination by a doctor.

What pathologies can lead to a child rarely urinating:
- The kidneys suffer, as a result of which their ability to produce the required amount of urine per day is lost.
- There was a partial blockage of the ureters (due to inflammation, infection, injury).
- The bladder is affected (often this is a consequence of a very long abstinence, when the child suffers, does not go to the toilet, and it constantly overflows).
- Sand or stones have formed in the bladder and kidneys.
- Compression of the urethra.
- The child experiences nervous tension, and as a result, hysteria, hypochondria, and fever due to nervousness set in.
- A new growth (benign or malignant) has appeared in the blood vessels.
- Pelvic tumors can cause obstruction of urine flow and urinary retention.
- Overdose. The child was treated incorrectly for another disease and was prescribed too many diuretics.
- The bladder has become distended.
- There were injuries to the head and lower spine.
- A hidden infection “wanders” in the genitourinary tract.
Norms of urination in a child per day
Before panicking, parents should find out what can be considered the daily urine output rate for a child.
The authoritative pediatrician A. Papayan, back in Soviet times, compiled a table with the norms of urine output according to the age of the child. This table still serves as the main guideline for many pediatricians when examining a child for the presence (absence) of pathology.
| Child's age | Daily urine volume, ml | Daily number of urinations | Volume of urine per urination, ml |
| 0-6 months | 300-500 | 20-25 | 20-35 |
| 6-12 months | 300-600 | 15-16 | 25-45 |
| 1-3 years | 760-820 | 10-12 | 60-90 |
| 3-5 years | 900-1070 | 7-9 | 70-90 |
| 5-7 years | 1070-1300 | 7-9 | 100-150 |
| 7-9 years | 1240-1520 | 7-8 | 145-190 |
| 9-11 years | 1520-1670 | 6-7 | 220-260 |
| 11-14 years old | 1600-1900 | 6-7 | 250-270 |
You need to worry if a child goes to the toilet much less often than his peers, although in this case the reason may not be dangerous at all.
What could be the reasons for rare urination in a child, and what can parents do?

Sometimes a child begins to pee less often because he is growing quickly or experiences inconvenience, getting used to new rules of personal hygiene: when switching from diapers to a potty.
| Age | Possible reason | What to do? |
| From birth to 12 | Completion of breastfeeding, transition to artificial nutrition | Mommy needs to ask all the necessary and unclear questions to the pediatrician. The pediatrician, in turn, when switching a child to artificial nutrition and/or introducing complementary foods, must tell him how to do this correctly, how much and how often to give the child water. Sometimes choosing the best food can be very difficult, and in the process of choosing, the little body experiences stress: this is why the baby rarely pees. |
| From birth to 3 months | Insufficient fat content of milk In addition to increased fat content of breast milk, there may be hypogalactia | Review your diet, introduce healthy fats, such as cheese or walnuts. Here you definitely need to consult a pediatrician: perhaps the problem is insufficient milk production in the mother (lactation crisis, stress, improper daily routine and poor nutrition). The pediatrician analyzes the mother's nutrition and, if necessary, makes adjustments; recommends taking a warm drink before each feeding (tea, compote, rosehip decoction). A bottle-fed baby, as a rule, does not experience such disadvantages, since the formula is as close in composition as possible to breast milk. |
| From 6 months to 12 | Introduction of complementary foods | Gradual introduction of complementary foods with foods and portions calculated by your pediatrician for your child. |
| From 9 months to 24 | Accustoming to a bottle, giving up a pacifier Accustoming to a bottle/sippy cup occurs earlier. Children with the introduction of complementary foods (and now recommended from 4 months) begin to be offered water in sippy cups, bottle-fed children - earlier: they drink from a teaspoon / through a bottle. | |
| From birth to 24 months | Insufficient drinking in the summer, especially hot periods | Go out for a walk only with a bottle of water and give it to your child upon request. |
| From 12 to 24 months | Refusal to use diapers, potty training | Try not to put pressure on the child and allow him to pee in the potty at will. Sometimes the training process begins with the banal choice of a potty that is attractive to the child. |
Transient hyperthermia in newborns
It also often becomes a serious cause for concern for parents. In this condition, the child’s body temperature may rise to 38.5-39.5 ° C and higher, the child may be restless, suckle greedily, have dry mucous membranes and other signs of dehydration. As a rule, transient hyperthermia occurs on the 3-5th day of life, and its frequency is 0.3-0.5%. Its development is facilitated by overheating, the location of the crib next to a central heating radiator or in direct sunlight, etc. The most common point of view on the cause of transient hyperthermia is dehydration. However, some authors associate it with the peculiarities of metabolism in newborns.
Tactics for transient hyperthermia boil down to physical cooling (the child is left free of clothing, of course, under the control of regular measurement of body temperature), and the establishment of breastfeeding. It has been noticed that the more often the baby is put to the breast and the more effectively he sucks the breast, the faster the baby’s body temperature normalizes. If the mother has delayed lactation or hypogalactia, then such a baby should not be kept on a starvation diet. This is also the rationale for prescribing formula to a child.